Leona Louise (Brooks) Reed, Quinter, passed away on July 17, 2019 at the age of 92 years, 10 months and 13 days. On September 4, 1926, Leona was born to Frank H. and Minnie L. (Kesler) Brooks in Quinter. She was joined later by a sister, who died in infancy, and two brothers. She grew up southwest of Quinter on the family farm and attended Sunshine School. Early in life, Leona joined the Dunkard Brethren Church and was a faithful member to the end.
Leona’s attention was drawn by aunts in Iowa and she moved there to work for a while. While there, she met William “Bill” Reed and they were married in Quinter on December 8, 1946. To this union, three daughters and two sons were born.
Leona was mostly a stay-at-home wife and mother but spent some years selling Fuller Brush products. She enjoyed her many customers along the way. While her children were home, Leona sewed their clothes. After they moved away, she began making beautiful quilts, wall hangings and many other crafts as well as creative picture albums. Later in life, one of her real joys was making beautiful greeting cards that she sent to family and friends. She would make around 150 cards per year.
In passing, Leona leaves William, her husband of 72 ½ years; daughters, Kathy Barker, Gayla (Wayne) Berens, Nancy (Tom) Stoltzfus; sons, Ross (Bridget) Reed, Lee (Connie) Reed; a brother, Marion (Joyce) Brooks; sister-in-law, Janis Millwee; 17 grandchildren; 20 great-grandchildren; cousins, nieces, nephews and friends. She was preceded in death by her parents, infant sister, Eunice, and brother, Merlin.
Funeral service will be 10:00 a.m., Wednesday, July 24, 2019, at the Dunkard Brethren Church, Quinter. Burial will be in the Baker Township Cemetery, Quinter.
Family hosted visitation will be Tuesday evening, from 6:00 to 8:00 p.m. at the church. There will be no public viewing.
Memorial contributions are suggested to Hospice Services, Inc. or Gideons International. Donations to the fund may be sent to Schmitt Funeral Home, 901 South Main, Quinter, KS 67752.
Father Mark A. Berland was born on December 14, 1948 to Fred and Eunice (Balthazor) Berland in Hays, Kansas. He was one of seven children and attended Zurich Public Schools until high school where he transferred to St. Francis Seminary in Victoria, Kansas. After graduating from high school he attended Conception Seminary College in Conception, Missouri and furthered his education at the Kenrick Theological Seminary School in St. Louis, Missouri. He was ordained into priesthood by Bishop Cyril Vogel on June 1, 1974 at the St. Ann Church in Zurich.
Father Mark Berland started his career as an associate pastor and assistant editor of “The Register” at the Sacred Heart Cathedral in Salina. Throughout his years he was posted as an associate pastor, head pastor, and religion teacher. In 2009 until his passing in 2019 he was the pastor at the Sacred Heart Parish in Oberlin, the Sacred Heart Parish in Selden, and the Immaculate Conception Parish in Leoville.
Father Mark not only enjoyed spreading the word of God but away from the church he enjoyed coin and stamp collecting as well as restoring old tractors.
He is survived by his mother Eunice (Balthazor) Berland, sisters; Kay and husband Chris Basgall of Owosso, MI, Ann and husband Tim Zwink of Piedmont, OK, Mary and husband Gary Everett of Wilson, KS, Lois Mason of Ellis, KS, and Rebecca and husband George Cobb of Peoria, AZ; brother-in-law Deacon Walt Slingsby, as well as nieces and nephews.
Father Mark is preceded in death by his father, Fred Berland, sisters Carol Slingsby and Joan Berland, and a brother-in-law Robert Mason.
A Vigil and Rosary will be held at the Sacred Heart Catholic Church in Plainville on Sunday, July 21, 2019, the visitation will run from 4:00pm until the Vigil beginning at 7:00pm with a Knights of Columbus rosary to follow. A Mass of Christian burial will be on Monday, July 22, 2019 starting at 11:00am at the Sacred Heart Catholic Church in Plainville, with a burial following at St. Ann’s Cemetery in Zurich. Memorials are suggested to the Retired Priests Fund – Salina Diocese and may be sent in care of Plumer-Overlease Funeral Home, 320 SW 2nd St, Plainville, KS 67663. Online condolences can be left at plumeroverlease.com
Just after 4p.m. Saturday, the Shawnee County Emergency Communications Center received a call about an injury accident that occurred at 117 NE highway 24, according to Lt. Robert Simmons.
When officers arrived they located what appeared to be a single vehicle accident with an adult male driver who was determined to be the sole occupant.
The man was initially unresponsive at the scene and was transported to an area hospital where he was pronounced deceased.
According to Simmons, it did not appear the man died from the accident.
Police do not believe the death to be suspicious in nature. He did not release the man’s name.
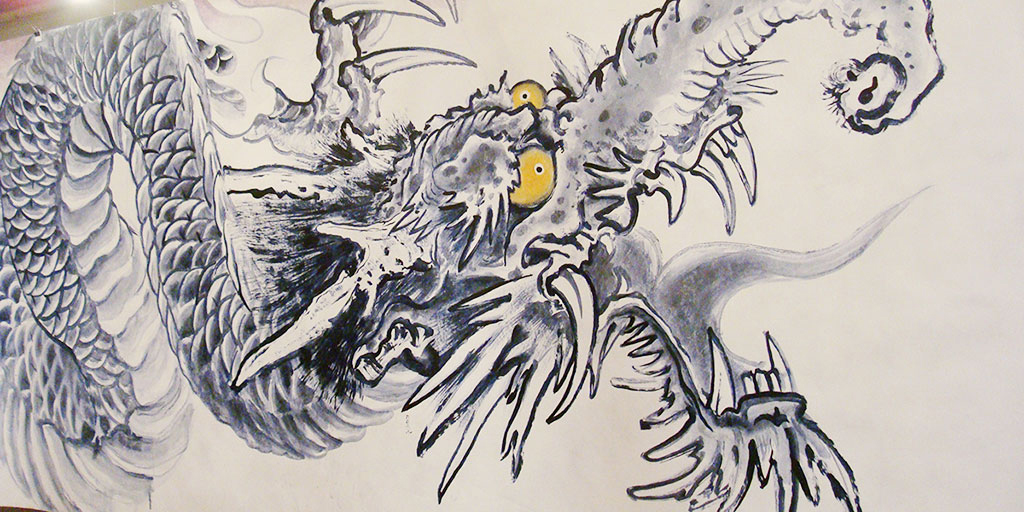
An excerpt from Hardy’s “2000 Dragons” scroll, taken during a 2012 exhibition at Diverse Works in Houston. (Courtesy Sherry Fowler)
KU NEWS SERVICE
LAWRENCE – Tattoo art icon Don Ed Hardy has come full circle more than once. He’s gone from student of East Asian art history to commercial juggernaut and back to fine art. And even within the fashion world, he’s had a recent comeback after his early 2000s success led to overexposure and backlash.
Sherry Fowler
As a friend of nearly 40 years, University of Kansas researcher Sherry Fowler was there for much of it. That’s partly why she, along with her husband, Dale Slusser, was asked to contribute an essay for the catalog that accompanies the forthcoming Hardy exhibition at San Francisco’s de Young Museum.
“Ed Hardy: Deeper Than Skin” (July 13-Oct. 6) is the first museum retrospective of the man known for elevating the tattoo from its subculture status to an important visual art form. The catalog is edited by curator Karin Breuer and published by Fine Arts Museums of San Francisco in association with Rizzoli Electa.
Fowler, KU professor of the history of art, said she met Hardy through his wife, Francesca Passalacqua, who was her Japanese-language classmate in San Francisco around 1980.
“One day she said, ‘I’ll give you a ride home, but I have to leave early because my husband’s going to be on ‘To Tell the Truth.’ That was a TV game show with three guests on it, two of whom were imposters, all who said that they were someone noteworthy or unusual — in this case the most famous tattoo artist in the United States,” Fowler said. “So I went home and watched the show. And I thought, ‘Well, which one is her husband?’ There were two old, salty sailor types, and then there was this young, cute guy, and I thought, ‘I hope it’s him.’ And it was. Panelist Kitty Carlisle got the answer right.”
Like her, Fowler said, Hardy loved and studied Asian art (he earned a Bachelor of Fine Arts with an emphasis in printmaking from the San Francisco Art Institute), and the couples became friends.
Slusser is associate vice president for development with KU Endowment and is an affiliate of the College of Liberal Arts & Sciences’ Center for East Asian Studies.
Just a few months ago, Hardy asked Fowler to write a catalog essay for the de Young show, and, with Slusser’s help, she agreed. The essay is titled “Drawing Embodied: Ed Hardy’s East Asian Art Connections.”
“The amazing thing about working on somebody who’s alive — you can actually email them and ask them questions,” said Fowler, who usually writes about premodern Japanese art. “But I was there for a lot of it, and I remember these things happening. Although I took care not to put myself in the narrative, I was thinking about it as I wrote.”
For instance, Fowler recalled, she served as interpreter for “the legendary Horiyoshi II” during the 1985 National Tattoo Association Convention in Seattle, an event mentioned in the catalog as one of many important milestones in Hardy’s career.
And while tattoo artists like Horiyoshi II, Horiyoshi III and Sailor Jerry Collins influential on Hardy’s tattoo style, so, too, was his training in East Asian art, Fowler argues in the catalog. It’s also apparent in his printmaking.
For instance, Fowler begins her essay by considering Hardy’s 2007 print titled “Our Gang.” It’s based on a bronze plaque dated to the year 1001 and held in the Tokyo National Museum. She said the central figure, known as Zao Gongen, “is a hybrid Shinto-Buddhist deity. And the print is emblematic of his career because it has so many different things going on, mixing very traditional Asian art with goofy stuff and personal things.”
Among the smaller figures surrounding the deity, Hardy has even depicted himself as a rat offering up a valentine heart to his wife, Fowler said. Fowler knew that among all the figures in the print there were portraits of Hardy and his wife, but she had to confirm with him which ones they were.
Fowler’s essay broaches the topic of cultural appropriation but in this specific case dismisses any bad intent on the part of the artist or any harm to his sources.
“I don’t think his work is for everybody,” Fowler said. “And sometimes I don’t like it when he pushes the envelope too far. But that is provoking. That makes us think and change our minds about certain things.”
Ultimately, Fowler said, it is the passion that undergirds Hardy’s style and technique that has made him a cultural force to be reckoned with.
“He loves art,” she said. “He is so passionate. He’s the kind of person who will get up in the morning and say, ‘I’ve been thinking about art all night; I couldn’t sleep.’ When you’re around him, you feel like you just want to make the most of every moment. You want to see everything. You want to do everything and experience as much art as you possibly can. He’s that kind of magnetic personality.”
While the Hardy show is at the de Young, there is a related show, “Tattoos in Japanese Prints,” at the Asian Art Museum in San Francisco.
“For a long time, there was a big stigma about tattooing, and now it’s everywhere,” Fowler said. “I think museums are making a real effort to connect to people, and so if you can have something historical that makes sense and connects to people’s lives, they will want to learn more about it.”
Kansas lawmakers may put the question of abortion rights to a public vote in 2020. CELIA LLOPIS-JEPSEN / KANSAS NEWS SERVICE
That means even if the U.S. Supreme Court overturns its 1973 Roe v. Wade ruling, lawmakers won’t be able to ban abortion in Kansas unless voters amend the state constitution.
But the matter remains far from settled. Here’s where things stand on abortion in Kansas, and some of the developments to keep an eye out for within state lines.
Abortions on the decline
A preliminary report from the state health department shows about 7,000 abortions took place in Kansas last year, about half of which involved patients from other states.
If that seems surprising, remember that the only abortion clinic in neighboring Missouri, for example, lies at the other end of that state in St. Louis (where it’s fighting for survival). The Kansas City metro area’s two abortion clinics both stand on the Kansas side of the border, in Overland Park.)
The annual number of abortions in Kansas has dropped significantly over the past few decades.
Nationally, abortion rates also have dropped, according to data collated by the Guttmacher Institute, a pro-abortion rights research center. Studies suggestsomewhere around a third of women in the U.S. get abortions by their mid-40s.
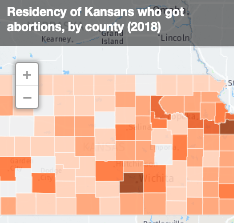
Who got abortions in 2018?
In Kansas, nearly a third of the women who had last year’s 7,000 abortions were in their early 20s. Nearly nine out of 10 were in their 20s or 30s. About one in six was married.
Though in-state abortions are only available at four clinics in Wichita and Overland Park, last year’s patients came from across the state.
Kansas has passed a slew of limits on abortion, particularly during Sam Brownback’s tenure as governor from 2011 through 2018. That includes a ban on abortions after the 22nd week of pregnancy unless medically necessary to protect the mother’s health.
About 70% of abortions in Kansas last year occurred within the first eight weeks of pregnancy. About 60% involved the “abortion pill,” nearly a third involved suction abortion and about 7% were dilation and evacuation abortions.
A constitutional amendment on the horizon?
Given the Kansas Supreme Court’s ruling, abortion foes may ask the public to tweak the state constitution, perhaps on the November 2020 ballot. That would require getting a bill through the state House and Senate with two-thirds majorities before getting to the public vote. Governors can’t veto constitutional amendment bills.
Supporters of changing the constitution have different ideas about how to do so. Lawmakers could potentially ask the public to ban all abortions, for example, or to bar the state’s courts from undoing abortion limits and bans that pass the Legislature.
Drug abortions by out-of-state doctors
The wheels have started turning again on a few old lawsuits making their way through the Kansas courts. At least one new lawsuit has cropped up this year, and more could be on the way.
The Kansas Supreme Court’s landmark ruling this spring about the right to abortion stemmed from a state ban on dilation and evacuation. (The ban wasn’t actually in effect, because courts had blocked it pending the case’s outcome.) Now the case bounces back to Shawnee County District Court, which will seal the fate of the dilation and evacuation ban based on the high court’s ruling. That could mean a whole new trial, which isn’t likely before 2020.
A Wichita abortion clinic says it can’t find local doctors and instead leans on physicians from other states.
Also at Shawnee County District Court: A Wichita abortion clinic that says it can’t find local doctors and instead leans on physicians from other states. It’s fighting to resume telemedicine abortions. (These are abortions in which the doctors work remotely with the clinic’s patients via video connection. They check whether the patient is eligible to take the abortion pill, and then guide the process.)
That legal battle involves two lawsuits and some very convoluted twists. In the simplest terms: A judge blocked the original 2011 ban on remote abortions years ago. The state, meanwhile, argues that the injunction shouldn’t apply anymore. And though a judge rejected that argument, the clinic is worried state agencies and local prosecutors won’t abide by his conclusions.
So the clinic hasn’t restarted the telemedicine abortions it stopped at the end of 2018 because it fears retaliation. As an example, it cites an ongoing investigation of its operations by the state agency in charge of medical licenses.
Other abortion restrictions on trial
Finally, litigation could undo a slew of other state restrictions related to abortion, including some that were temporarily blocked by the courts and others that were allowed to take effect.
Just a few of the restrictions targeted in ongoing lawsuits from 2011 and 2013:
Faculty from the state’s only school of medicine can’t teach their students how to perform abortions either on or off university property.
Women must wait 24 hours for an abortion even if the delay would kill them, according to the plaintiffs’ reading of a 2013 law. They say lawmakers tweaked the state’s exceptions such that no emergency can pass their test.
Clinics must deliver a number of messages to patients discouraging abortion. They include hanging a message that plaintiffs argued takes 6 square feet to print in the Legislature’s chosen font size.
Under a 2011 law, doctors need another person in the room when giving a pelvic exam to a patient who wants an abortion, even if the patient doesn’t want anyone else present.
Plaintiffs also argue related regulations grant state health workers access to the individual medical records of women who’ve had abortions.
Clinics must do urine tests to check whether a woman’s abortion worked or whether she remains pregnant. Plaintiffs argue urine tests are less accurate than the ultrasounds and physical exams that doctors normally use.
And since Kansas has plenty of other restrictions on the books, too, such as that ban on most abortions after 22 weeks, future lawsuits based on this spring’s Kansas Supreme Court ruling could be in the pipeline.
Celia Llopis-Jepsen reports on consumer health and education for the Kansas News Service. You can follow her on Twitter @Celia_LJ or email her at celia (at) kcur (dot) org.
Gov. Laura Kelly appointed 13 members to the Alzheimer’s Disease Task Force.
This task force assesses the current and future impact of Alzheimer’s disease on Kansas residents; examines the existing industries, services, and resources addressing the needs of people with Alzheimer’s, their families, and caregivers; and develops a strategy to mobilize a state response to the public health crisis.
“Alzheimer’s disease touches so many lives, and we must do what we can to help patients and their families cope with this tragic ailment,” Kelly said. “I appreciate the interest from all willing to serve on this important task force.”
The appointed task force members:
1. Jamie Gideon, Haysville – Chair 2. Cindy Schmidt, Hays
3. Gina Long, Gardner
4. Rita Ortolani, Independence
5. Robert Miller, Wichita
6. Sarah Duggan, Manhattan
7. Steve Harader, Wichita
8. Dr. Joseph G. Schlageck, Overland Park
9. Janie Krull, Wichita
10. Dr. Stephen Benson, Wichita 11. Randy Clinkscales, Hays
12. Carol Jolly, Topeka
13. Rob Razo, Topeka
The task force meets monthly or as needed at the discretion of the Chair.
The task force will receive data, research, administrative support and guidance from the following agencies: Kansas Department of Labor, Kansas Department of Commerce, Kansas Department for Aging and Disability Services, and the Kansas Department of Health and Environment. The Kansas Department for Aging and Disability Services shall be primarily responsible for and take the lead in providing support.
The Task Force is directed to submit a report of its findings and recommendations to the Legislature and Governor in the form of a Kansas Alzheimer’s Disease Plan by Jan. 13 or as appropriate during the intervening period.
A slight chance of showers and thunderstorms before 3pm, then a slight chance of showers and thunderstorms after 5pm. Partly sunny, with a high near 87. North northeast wind 9 to 13 mph. Chance of precipitation is 20%.
Sunday Night
A 30 percent chance of showers and thunderstorms, mainly before 1am. Mostly cloudy, with a low around 60. North northeast wind 14 to 17 mph.
Monday
Partly sunny, then gradually becoming sunny, with a high near 82. North northeast wind 13 to 15 mph.
Monday Night
Clear, with a low around 55. Northeast wind 9 to 14 mph becoming light east northeast in the evening.
RUSSELL COUNTY — The Kansas Department of Transportation will temporarily close a portion of U.S. 281 north of the city of Russell starting Monday, July 22.
The highway will be closed to through traffic between Shoreline Road and Land Road, or from milepost 146 to 149, for crews to make partial repairs to a slide area that has affected the roadway. KDOT expects to reopen the road to one-lane traffic controlled by a traffic signal by the end of the week, weather permitting. The traffic signal configuration will remain in place until further repairs can be made and be removed once the additional work is completed.
Travelers are advised to utilize state routes K-18, K-232 and I-70 as an easterly route around the closure, and K-18, U.S. 183 and I-70 as a westerly route around the closure.
American College of Cardiology NCDR Chest Pain̶MI Registry Platinum Award recognizes high standards of patient care
HaysMed has received the American College of Cardiology’s NCDR Chest Pain̶MI Registry Platinum Performance Achievement Award for 2019. HaysMed is one of only 225 hospitals nationwide to receive the honor.
The award recognizes HaysMed’s commitment and success in implementing a higher standard of care for heart attack patients and signifies that HaysMed has reached an aggressive goal of treating these patients to standard levels of care as outlined by the American College of Cardiology/American Heart Association clinical guidelines and recommendations.
To receive the Chest Pain̶ MI Registry Platinum Performance Achievement Award, HaysMed has demonstrated sustained achievement in the Chest Pain̶ MI Registry for eight consecutive quarters and has performed at the top level of standards for specific performance measures. Full participation in the registry engages hospitals in a robust quality improvement process using data to drive improvements in adherence to guideline recommendations and overall quality of care provided to heart attack patients.
“As a Platinum Performance Award recipient, HaysMed has established itself as a leader in setting the national standard for improving quality of care in patients with acute myocardial infarction,” said Michael C. Kontos, MD, FACC, chair of the NCDR Chest Pain – MI Registry Steering Subcommittee, Virginia Commonwealth University Medical Center. “By meeting the award requirements set forth in the registry, HaysMed has demonstrated a commitment to providing reliable, comprehensive treatment for heart attack patients based on current clinical guideline recommendations.”
The Center for Disease Control estimates over 700,000 Americans suffer a heart attack each year. A heart attack occurs when a blood clot in a coronary artery partially or completely blocks blood flow to the heart muscle. Treatment guidelines include administering aspirin upon arrival and discharge, timely restoration of blood flow to the blocked artery, smoking cessation counseling and cardiac rehabilitation, among others.
“This award reflects the ongoing commitment of DeBakey Heart Institute, HaysMed, and the University of Kansas health system to the goal of improving the cardiovascular health of our patients in western and central Kansas. Congratulations to all involved!” said Jeffery Curtis, FACC, FACP, director of Cardiology Services.
Chest Pain̶MI Registry empowers health care provider teams to consistently treat heart attack patients according to the most current, science-based guidelines and establishes a national standard for understanding and improving the quality, safety and outcomes of care provided for patients with coronary artery disease, specifically high-risk heart attack patients.
The American College of Cardiology envisions a world where innovation and knowledge optimize cardiovascular care and outcomes. As the professional home for the entire cardiovascular care team, the mission of the college and its more than 52,000 members is to transform cardiovascular care and to improve heart health. The ACC bestows credentials upon cardiovascular professionals who meet stringent qualifications and leads in the formation of health policy, standards and guidelines. The college also provides professional medical education, disseminates cardiovascular research through its world-renowned JACC Journals, operates national registries to measure and improve care, and offers cardiovascular accreditation to hospitals and institutions. For more, visit acc.org.
When the cancer clinic at Mercy Hospital Fort Scott closed in January 2019, cancer patients such as Karen Endicott-Coyan had to continue their treatment in different locations. Endicott-Coyan has a rare form of multiple myeloma and now drives an hour from her farm near Fort Scott to Chanute for weekly chemotherapy injections. (Christopher Smith for KHN)
One Monday in February, 65-year-old Karen Endicott-Coyan gripped the wheel of her black 2014 Ford Taurus with both hands as she made the hour-long drive from her farm near Fort Scott to Chanute. With a rare form of multiple myeloma, she requires weekly chemotherapy injections to keep the cancer at bay.
She made the trip in pain, having skipped her morphine for the day to be able to drive safely. Since she sometimes “gets the pukes” after treatment, she had her neighbor and friend Shirley Palmer, 76, come along to drive her back.
Continuity of care is crucial for cancer patients in the midst of treatment, which often requires frequent repeated outpatient visits. So when Mercy Hospital Fort Scott, the rural hospital in Endicott-Coyan’s hometown, was slated to close its doors at the end of 2018, hospital officials had arranged for its cancer clinic — called the “Unit of Hope” — to remain open.
Then “I got the email on Jan. 15,” said Reta Baker, the hospital’s CEO. It informed her that Cancer Center of Kansas, the contractor that operated and staffed the unit, had decided to shut it down too, just two weeks later.
“There are too many changes in that town” to keep the cancer center open, Yoosaf “Abe” Abraham, chief operating officer of the Cancer Center of Kansas, later told KHN. He added that patients would be “OK” because they could get treated at the center’s offices in Chanute and Parsons.
From Fort Scott, those facilities are 50 and 63 miles away, respectively.
For Endicott-Coyan and dozens of other cancer patients, the distance meant new challenges getting lifesaving treatment. “You have a flat tire, and there is nothing out here,” Endicott-Coyan said, waving her arm toward the open sky and the pastures dotted with black Angus and white-faced Hereford cattle on either side of the shoulderless, narrow highway she now must drive to get to her chemo appointment.
Nationwide, more than 100 rural hospitals have closed since 2010. In each case, a unique but familiar loss occurs. Residents, of course, lose health care services as wards are shut and doctors and nurses begin to move away.
But the ripple effect can be equally devastating. The economic vitality of a community takes a blow without the hospital’s high-paying jobs and it becomes more difficult for other industries to attract workers who want to live in a town with a hospital. Whatever remains is at risk of withering without the support of the stabilizing institution.
The 7,800 residents of Fort Scott are reeling from the loss of their 132-year-old community hospital that was closed at the end of December by Mercy, a St. Louis-based nonprofit health system. Founded on the frontier in the 19th century and rebuilt into a 69-bed modern facility in 2002, the hospital had outlived its use, with largely empty inpatient beds, the parent company said. For the next year, Kaiser Health News and NPR will track how its citizens fare after the closure in the hopes of answering pressing national questions: Do citizens in small communities like Fort Scott need a traditional hospital for their health needs? If not a hospital, what then?
Reta Baker, the hospital’s president who grew up on a farm south of Fort Scott, understood that the hospital’s closure was unavoidable. She scrambled to make sure basic health care needs would be met. Mercy agreed to keep the building open and lights on until 2021. And Baker recruited a federally qualified health center to take over four outpatient clinics, including one inside the hospital; former employees were bought out and continue to operate a rehabilitation center; and the nonprofit Ascension Via Christi Hospital in Pittsburg reopened the emergency department in February.
But cancer care in rural areas, which requires specialists and the purchase and storage of a range of oncology drugs, presents unique challenges.
Rural cancer patients typically spend 66% more time traveling each way to treatment than those who live in more urban areas, according to a recent national survey by ASCO, the American Society of Clinical Oncology. Dr. Monica Bertagnolli, a cattle rancher’s daughter who is now chair of ASCO’s board, called this a “tremendous burden.” Cancer care, she explained, is “not just one visit and you’re done.”
ASCO used federal data to find that while about 19% of Americans live in rural areas, only 7% of oncologists practice there.
People in rural America are more likely to die from cancer than those in the country’s metropolitan counties, according to a Centers for Disease Control and Prevention report in 2017. It found 180 cancer deaths per 100,000 people a year in rural counties, compared with 158 deaths per 100,000 in populous metropolitan counties.
The discrepancy is partly because habits like smoking are more common among rural residents, but the risk of dying goes beyond that, said Jane Henley, a CDC epidemiologist and lead author of the report. “We know geography can affect your risk factors, but we don’t expect it to affect mortality.”
From an office inside a former Mercy outpatient clinic, Fort Scott’s cancer support group, Care to Share, continues its efforts to meet some of the community’s needs — which in some ways have increased since the Unit of Hope closed. It provides Ensure nutritional supplements, gas vouchers and emotional support to cancer patients.
Lavetta Simmons, one of the support group’s founders, said she will have to raise more money to help people pay for gas so they can drive farther to treatments. Last year, in this impoverished corner of southeastern Kansas, Care to Share spent more than $17,000 providing gas money to area residents who had to travel to the Mercy hospital or farther away for care.
According to the U.S. Centers for Disease Control and Prevention, cancer kills more people in rural America than in the country’s metropolitan counties — 180 deaths per 100,000 people versus 158 deaths per 100,000 people. (Sara Jane Tribble/KHN)
The group expects to spend more on gas this year, having spent nearly $6,000 during the first four months of 2019.
And the reserves of donated Ensure from Mercy are running out, so Simmons is reaching out to hospitals in nearby counties for help.
With Mercy Hospital Fort Scott closed, the likelihood of residents here dying from their cancer will grow, experts worry, because it’s that much harder to access specialists and treatments.
Krista Postai, who took over the Fort Scott hospital’s four primary care clinics, said it’s not unusual for her staff to “see someone walk in [with] end-stage cancer that they put off because they didn’t have money, they didn’t have insurance, or it’s just the way you are. … We wait too long here.”
‘If they can’t cure me, I’m done’
Art Terry, 71, a farmer and Vietnam veteran, was one of them. Doctors discovered Terry’s cancer after he broke a rib while baling hay. When they found a mass below his armpit, it was already late-stage breast cancer that had metastasized to his bones.
With his twice-weekly chemotherapy treatment available in the “Unit of Hope,” Terry spent hours there with his son and grandchildren telling stories and jokes as if they were in their own living room. The nurses began to feel like family, and Terry brought them fresh eggs from his farm.
“Dad couldn’t have better or more personalized care anywhere,” said his son, Dwight, bleary-eyed after a factory shift.
Art Terry, center, stands for a family photo at the Mercy Hospital Fort Scott cancer unit before its January closure. From left are Terry’s daughter-in-law, Sabrina; granddaughters Aubry and Shaylee; son Dwight; and grandson Blaiton. (Courtesy Dwight Terry)
Terry knew it was difficult to find trustworthy cancer care. The shortage of cancer specialists in southeastern Kansas meant that many, including Mercy Hospital Fort Scott’s patients, counted on traveling oncologists to visit their communities once or twice a week.
Wichita-based Cancer Center of Kansas has nearly two dozen locations statewide. It began leasing space in Fort Scott’s hospital basement in the mid-2000s, the center’s Abraham said. The hospital provided the staff while the Cancer Center of Kansas paid rent and sent roving oncologists to drop in and treat patients.
At its closing, the Unit of Hope served nearly 200 patients, with about 40% of them on chemotherapy treatment.
When Art Terry was diagnosed, his son tried to talk to him about seeking treatment at the bigger hospitals and academic centers in Joplin, Mo., or the Kansas City area. The elder Terry wasn’t interested. “He’s like, ‘Nope,’” Dwight Terry recalled. “I’m going right there to Fort Scott. If they can’t cure me, I’m done. I’m not driving.’”
In the end, as the elder Terry struggled to stay alive, Dwight Terry said he would have driven his father the hour to Chanute for treatment. Gas — already a mounting expense as they traveled the 20 miles from the farm near tiny Prescott, Kan., to Fort Scott — would be even more costly. And the journey would be taxing for his father, who traveled so little over the course of his life that he had visited Kansas City only twice in the past 25 years.
As it turned out, the family never had to make a choice. Art Terry’s cancer advanced to his brain and killed him days before the hospital’s cancer unit closed.
What happens next?
Debbie Endicott, Karen Endicott-Coyan’s sister-in-law, drives to chemotherapy in Chanute. The trip takes an hour on mostly narrow, two-lane highways from Endicott-Coyan’s home south of Fort Scott. ‘You can see there are no gas stations, there is nothing in the way,’ Endicott-Coyan says. ‘There isn’t anything.’ (Sara Jane Tribble/ KHN)
As Endicott-Coyan and her friend Palmer drove to Chanute for treatment, they passed the time chatting about how the hospital’s closure is changing Fort Scott. “People started putting their houses up for sale,” Palmer said.
Like many in Fort Scott, they had both spent their days at the Fort Scott hospital. Endicott-Coyan worked in administration for more than 23 years; Palmer volunteered with the auxiliary for six years.
The hospital grew with the community. But as the town’s fortunes fell, it’s perhaps no surprise that the hospital couldn’t survive. But the intertwined history of Mercy and Fort Scott is also why its loss hit so many residents so hard.
Fort Scott began in 1842 when the U.S. government built a military fort to help with the nation’s westward expansion. Historians say Fort Scott was a boomtown in the years just after the Civil War, with its recorded population rising to more than 10,000 as the town competed with Kansas City to become the largest railroad center west of the Mississippi. The hospital was an integral part of the community after Sisters of Mercy nuns opened a 10-bed hospital in 1886 with a mission to serve the needy and poor. Baker, Mercy Hospital Fort Scott’s president, said the cancer center was an extension of that mission.
The Unit of Hope began operating out of the newest hospital building’s basement, which was “pretty cramped,” Baker said. As cancer treatments improved, it grew so rapidly that Mercy executives moved it to a spacious first-floor location that had previously been the business offices.
“Our whole purpose when we designed it was for it to be a place where somebody who was coming to have something unpleasant done could actually feel pampered and be in a nice environment,” Baker said.
The center, with its muted natural grays and browns, had windows overlooking the front parking lot and forested land beyond. Every patient could look out the windows or watch their personal television terminal, and each treatment chair had plenty of space for family members to pull up chairs.
Karen Endicott-Coyan and her husband, John Coyan, laugh while sitting in their kitchen. John, 74, began showing signs of dementia in 2015. Together, they run a cow-calf operation on 240 acres south of Fort Scott and go to church every Sunday. (Christopher Smith for Kaiser Health News)
When Endicott-Coyan and Palmer arrived at the Cancer Center of Kansas clinic in Chanute in February, things looked starkly different. Patients entered a small room through a rusted back door. Three brown infusion chairs sat on either side of the entry door and two television monitors were mounted high on the walls. A nurse checked Endicott-Coyan’s blood pressure and ushered her back to a private room to get a shot in her stomach. She was ready to leave about 15 minutes later.
The center’s Abraham said the Chanute facility is “good for patients for the time being” and not a “Taj Mahal” like Mercy’s Fort Scott hospital building, which he said was too expensive to maintain. Cancer Center of Kansas plans to open a clinic at a hospital in Girard, which is about 30 miles from Fort Scott, he said.
Some oncology doctors would say driving is not necessary. Indeed, a few health care systems across the country, such as Sanford Health in South Dakota and Thomas Jefferson University Hospitals in Pennsylvania, are administering some chemotherapy in patients’ homes. Oncologist Adam Binder, who practices at Thomas Jefferson in Philadelphia, said “over 50% of chemotherapy would be safe to administer in the home setting if the right infrastructure existed.”
But the infrastructure — that is, the nurses who would travel to treat patients and a reimbursement model to pay for such care within our complex health care system — is not yet in place.
Back in the car, Palmer took the wheel and Endicott-Coyan began planning for future cancer treatments in the void left by Mercy Hospital Fort Scott’s closure. “I put a note on Facebook today and said, ‘OK, I have drivers for the rest of February; I need drivers for March!’”
This is the first installment in KHN’s year-long series, No Mercy, which follows how the closure of one beloved rural hospital disrupts a community’s health care, economy and equilibrium.

 Leona Louise (Brooks) Reed, Quinter, passed away on July 17, 2019 at the age of 92 years, 10 months and 13 days. On September 4, 1926, Leona was born to Frank H. and Minnie L. (Kesler) Brooks in Quinter. She was joined later by a sister, who died in infancy, and two brothers. She grew up southwest of Quinter on the family farm and attended Sunshine School. Early in life, Leona joined the Dunkard Brethren Church and was a faithful member to the end.
Leona Louise (Brooks) Reed, Quinter, passed away on July 17, 2019 at the age of 92 years, 10 months and 13 days. On September 4, 1926, Leona was born to Frank H. and Minnie L. (Kesler) Brooks in Quinter. She was joined later by a sister, who died in infancy, and two brothers. She grew up southwest of Quinter on the family farm and attended Sunshine School. Early in life, Leona joined the Dunkard Brethren Church and was a faithful member to the end.























 Sunday
Sunday








